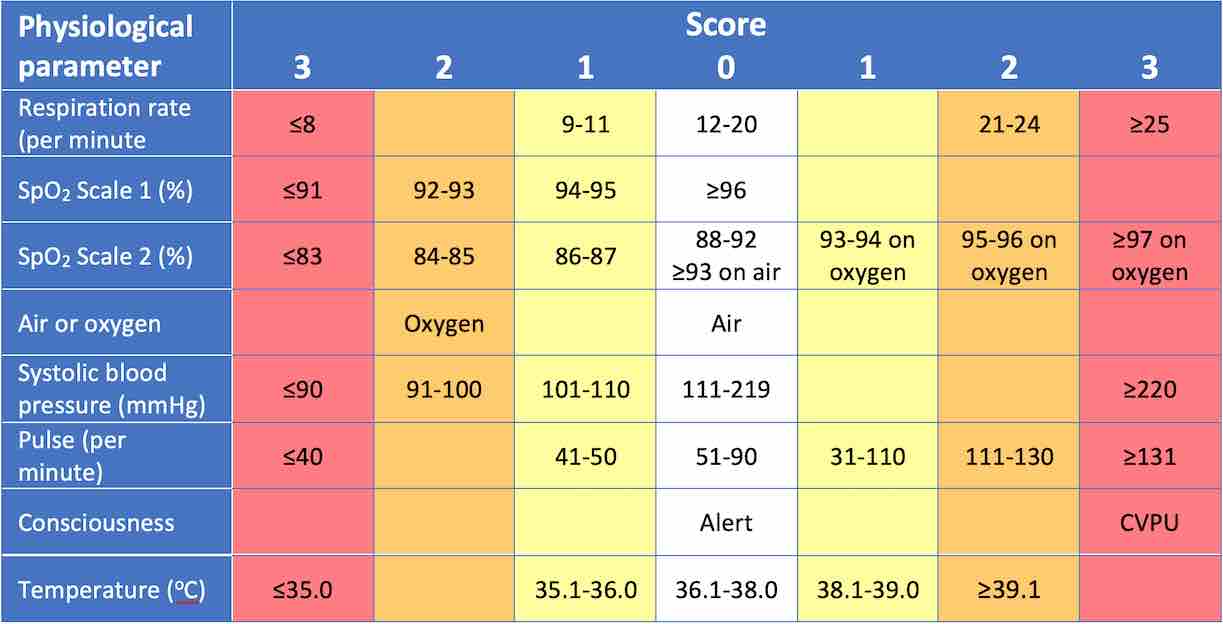
Basic observations are an essential part of assessment and detection of clinically deteriorating patients. NHS England advocates the use of the National Early Warning Score 2 (NEWS2) for assessment of adult patients in acute and ambulance settings. This page will cover the techniques required to complete this assessment.
Introduce yourself to the patient with your name and role, and confirm the patients name and date of birth. Explain that you are about to take some basic observations and obtain consent. Wash your hands.
If the patient is confused or unconscious, check their identity from their hospital wrist band.
Respiratory rate
Record the number of inspirations over a 30 second period. Multiple this by two to get the respiratory rate per minute.
A raised respiratory rate per minute (>20) or hyperventilation may be physiological, such as post-exercise or otherwise can be suggestive of hypoxaemia (low blood oxygen concentration), shock, metabolic acidosis, anxiety or stress.
A reduced respiratory rate per minute (<12), or hypoventilation can by caused by physical limitations such as chest trauma, obesity, obstructive sleep apnoea and neuromuscular disorders (such as myaesthenia gravis or Guillain Barré syndrome) or metabolic causes such as metabolic alkalosis, central nervous system depressants (alcohol and narcotics), brainstem stroke and severe hypothyroidism. Hyperoxia (over-oxygenation) in COPD will lead to a relative hypoventilation (see “hyperoxia in COPD” box in the next section).
Oxygen saturation
Attach a pulse oximeter to the patient’s index finger to record the patient’s blood oxygen saturation. This records the percentage of haemoglobin binding sites occupied by oxygen in the body. Normal oxygen saturation is 96% and above. Record whether or not the patient is receiving any oxygen and if so, then at what flow rate.
A low oxygen saturation (<96%) is almost always due to hypoxaemia (low blood oxygen concentration) as there is less oxygen available to bind to the haemoglobin. The most common cause of hypoxaemia is hypoxia (inadequate tissue oxygen) of the lung such as in COPD, asthma or pneumonia. Other causes include hypoventilation, high altitude, ventilation-perfusion mismatch (such as in pulmonary embolism [PE]) or left-to-right shunting of blood.
In patients with COPD, aim for a target of 88-92% as over-oxygenating these patients may lead to hypercapnia (high levels of blood carbon dioxide [CO2]).
A pulse oximeter measures the amount of red and infrared light waves absorbed by oxygenated haemoglobin in the blood. As a result, an accurate reading is dependent on good, peripheral vascular flow. If you are unable to get a reading with a finger pulse oximeter you may need to switch to an ear lobe pulse oximeter instead.
When recording a patient’s oxygen saturation, it is important to state how much oxygen the patient is receiving. In the UK, this is measured as “flow rate” and ranges from 1-15L per minute. A patient receiving no oxygen will be inhaling room air which is made up of 21% oxygen. A patient on oxygen will be inhaling both oxygen and room air, and so the fraction of oxygen inhaled will be dependent on the flow rate and the mode of delivery. For example:
A patient receiving 100% oxygen at 1L/minute via nasal cannulae will be inhaling roughly 24% oxygen.
A patient receiving 100% oxygen at 4L/minute via nasal cannulae will be inhaling roughly 36% oxygen.
A patient receiving 100% oxygen at 15L/minute via a non-rebreather mask will be receiving >90% oxygen.
A patient receiving 100% oxygen at 4L/minute via a blue venturi mask will be inhaling roughly 24% oxygen.
Ventilation-perfusion (V/Q) mismatch is a situation in which well-ventilated areas of lung receive insufficient blood supply whilst poorly-ventilated areas receive good blood supply. The body tries to avoid VQ mismatches by hypoxic vasoconstriction, a mechanism in which lung hypoxia causes vasoconstriction of arterioles supplying blood to that area.
The respiratory drive that serves to influence the ventilatory muscles is partly determined by the central chemoreceptors in the medulla oblungata. Hypercapnia, hypoxaemia and a low pH will act to increase respiratory drive. Blood CO2 combines with water to form carbonic acid – thereby reducing blood pH and causes a respiratory acidosis. In patients with longstanding COPD there are certain changes to the body as follows:
Due to the bronchitis and emphysematous effects, there will be certain areas of the lung which struggle to ventilate, and thus oxygenate sufficiently. The body compensates for this by hypoxic vasoconstriction, diverting blood from these hypoxic areas to better ventilated ones.
The kidneys act to compensate for the respiratory acidosis and over time the pH normalises. In addition, the central chemoreceptors become less responsive to hypercapnia, and so increased CO2 levels will not be met with a satisfactory increase in ventilation.
With the above points in mind, if you increase the fraction of inhaled oxygen such that they entire lung is well oxygenated (or over-oxygenated in this case) the following problems develop:
Ventilation-perfusion mismatch: The hypoxic vasoconstriction effect will be nullified and blood will flow to poorly ventilated areas. CO2 will struggle to escape from these areas and the degree of hypercapnia will increase, without any increase in ventilatory rate.
Haldane effect: Deoxygenated haemoglobin binds well to CO2. Lung hyperoxia will cause an increase in oxygenated haemoglobin. This leads to a “rightward” shift of the CO2 dissociation curve known as the Haldane effect. The degree of hypercapnia will increase, without any increase in ventilatory rate.
As a result, the NEWS2 suggests maintaining blood oxygen saturation in patients with COPD and chronic hypercapnia between 88-92% in order to prevent hyperoxia and any subsequent worsening hypercapnia.
Methaemoglobinaemia is a rare condition in which there is an excessive amount of methaemoglobin in the blood. Methaemoglobin is a form of haemoglobin where the iron has been converted from its ferrous (Fe2+) form to its ferric (Fe3+) form. This may be triggered by certain medications. Patients with a deficiency of methaemoglobin reduction enzyme (NADH-cytochrome b5 reductase) - such as those with a genetic deficiency or those under 6 months of age - are more susceptible to the condition.
It will present with a low blood oxygen saturations despite there being no evidence of hypoxaemia (i.e. there is a normal arterial oxygen level).
Systolic blood pressure
Record the patient’s blood pressure at rest. To do this, you will need:
Sphygmomanometer (manual blood pressure cuff).
Stethoscope
Ensure the patient’s preferred arm is placed comfortably at around heart level. Check that you are using the correct size cuff and that is it deflated (by opening the valve).
Palpation
Palpate for the brachial pulse, medial to the biceps brachii tendon. Line up the arrow marked on the cuff with the brachial artery and fasten the cuff around the patient’s arm.
Ensure that the valve is closed on the hand pump. Inflate the cuff whist palpating the radial pulse. At the point where you can no longer feel the pulse, read the meter; this is a rough estimate of the patient’s systolic blood pressure.
Deflate the cuff and close the valve again. Place the diaphragm of your stethoscope over the brachial pulse, just under the cuff.
Place the diaphragm just under the cuff.
Auscultation
Inflate the cuff to 20mmHg above your estimated systolic pressure. Next, by minimally opening the valve, slowly deflate at around 2-3mmHg/s, whilst watching the pressure dial.
Listen carefully for loud beating sounds called ‘Korotkoff sounds.’ When you first hear the sounds, read the meter; this will be the systolic pressure. You will continue to hear the sounds for a brief amount of time. Once the sounds have completely died away, read the meter again; this will be the diastolic pressure. Readings are usually taken to the nearest 2mmHg.
Palpate the radial pulse, just lateral to the tendon of the flexor carpi radialis. Record the number of beats over 15 seconds and multiple by 4 to give you the pulse rate (heart rate) per minute . If you are unable to palpate the radial pulse, then palpate the carotid pulse just anterior to the sternocleidomastoid muscle, underneath the angle of the jaw.
A raised pulse per minute (>100) or tachycardia may be physiological, such as post-exercise or otherwise may be secondary to fever, infection, arrythmia, shock, pulmonary hypertension (including PE), hyperthyroidism, fear/anxiety or stress.
A reduced pulse per minute (≤60), or bradycardia may also be physiological in fit patients who do a lot of aerobic exercise. Pathological causes include heart disease (such as ischaemia or heart block), hypothyroidism and certain medications such as beta-blockers.
A pulse oximeter will also measure the patient’s pulse rate per minute.
Note that the NEWS2 score scores tachycardia at >90 and bradycardia as ≤50 (pulse per minute).
Consciousness
Talk to the patient and assess their response via the ACVPU scale. If the patient is asleep, then you will need to wake them up:
Alert: The patient is fully responsive to voice and has motor function.
Confused: The patient is fully responsive to voice however they are agitated or disorientated.
Voice: The patient makes a minimal response to voice by opening their eyes, making sounds or moving.
Pain: The patient makes a minimal response to pain by opening their eyes, making sounds or moving.
Unconscious: The patient makes no response to pain.
A more detailed assessment of consciousness is the Glasgow Coma Scale which more accurately assesses the patient’s ocular, verbal and motor responses to interaction.
Temperature
There are numerous methods of recording temperature:
Tympanic: Using a clean probe, place the device in the patient’s ear and gently pull on the ear lobe to straighten the external auditory canal. Gently insert the thermometer and record the temperature. Dispose of the probe. This is the most common method used for adults in UK hospitals as it is easy and cheap to replace the probe.
Oral: Carefully place the tip of the thermometer under the patient’s tongue and record the temperature. Dispose of the thermometer.
Axillary: Carefully place the tip of the thermometer in the centre of the patient’s axilla. Ask them to place their hands by their side such that the thermometer is held in place. Record the reading and then dispose of the thermometer.
A raised temperature (>38℃) or pyrexia may be caused by infection, inflammatory disease, cancers and drugs.
A reduced temperature (≤36℃) or hypothermia may be due to prolonged exposure to cold water or weather or caused by alcohol intoxication, certain medications and hypothyroidism.
Temperature may also be measured rectally, however this is only ever used in newborn babies, if at all, and should only be done by those who are trained to do so.
Completion
Ensure that your observations are recorded in the patient’s notes or observation chart. If you are using the NEWS2 system, use the scoring table to determine their NEWS2 score and take the following actions:
0: Continue monitoring at a minimum rate of 12-hourly
1-4: Inform a registered nurse who must assess whether further escalation is required. Continue monitoring 4-6 hourly.
3 in a single parameter: A registered nurse should contact the medical team to determine whether a review +/- escalation of care is necessary. Continue to monitor every hour.
5-6: A registered nurse should contact the medical team and request an urgent review by a clinician or critical care practitioner. Continue to monitor every hour. Consider moving patient to an area with continuous monitoring facilities.
7+: A registered nurse should contact the medical team and a specialist registrar or consultant should be informed. Request an urgent review by a senior clinician or critical care practitioner. Start continuous monitoring. Consider transfer to a high-dependency or intensive care unit.
Interactive markscheme
When assessing each other, click on each list item as you go along. Doing so will turn the list item green. Make careful note of any steps missed at the end. We recommend completing any examination or procedure in under 10 minutes, but you can adjust the timer to suit your needs.
:
Introduction: “Hello, I’m SimpleOSCE and I am a medical student. Today I’ve been asked to take some basic observations from you. Can I confirm your name and DOB? Thank you.”
Obtain consent.
Wash your hands.
Record respiratory rate per minute over 30 seconds.
Use a pulse oximeter to record blood oxygen saturation.
Record the patient’s blood pressure.
Record the pulse rate per minute over at least 15 seconds.
Record consciousness via the ACVPU scale.
Record the patient’s temperature by tympanic, oral or axillary means.
Document your findings in the patients notes, using the NEWS2 score or otherwise.