Introduce yourself to the patient and confirm the patient’s name and date of birth. Obtain consent and proceed to wash your hands.
General inspection
Begin the examination by inspecting the patient. They will need to be exposed entirely above and below the waist. Patients may keep their undergarments on but should remove their shoes and socks.
Ask the patient if they are comfortable or in any pain. Look around the bed for any items/clues such as walking aids or medications.
This level of exposure can be uncomfortable for some patients. Throughout the examination, make an effort to ensure that the patient is comfortable in the environment and that their dignity is maintained.
Whilst the patient is removing their garments you can make observations as to their general ability to mobilise and also observe the wear pattern of their shoes.
Screening questions
Before advancing any further, you must ask the patient three screening questions. These will give you an idea of the patient’s issues with mobility or the impact of pathology on their life. It also enables you to identify any painful regions of their musculoskeletal system which you should be careful with during your examination.
1. “Do you have any pain or stiffness in any of your joints, in your muscles, or in your back?”
2. “Do you experience any difficulty with walking up and down stairs?”
3. “Do you experience any difficulty with dressing yourself in the morning?”
These three questions address the main features of musculoskeletal disorders: pain, stiffness, swelling and functional impairment.
1. This addresses any notable symptoms the patient has identified with their musculoskeletal system and will help you to make sense of your findings.
2. This assesses gross motor function with respect to the patient’s muscle bulk. Issues with walking up and down stairs may indicate muscle wasting in the lower limb (affecting leg movement) and thorax (affecting posture).
3. This crudely assesses fine motor function of the patient and their joints.
Closer inspection
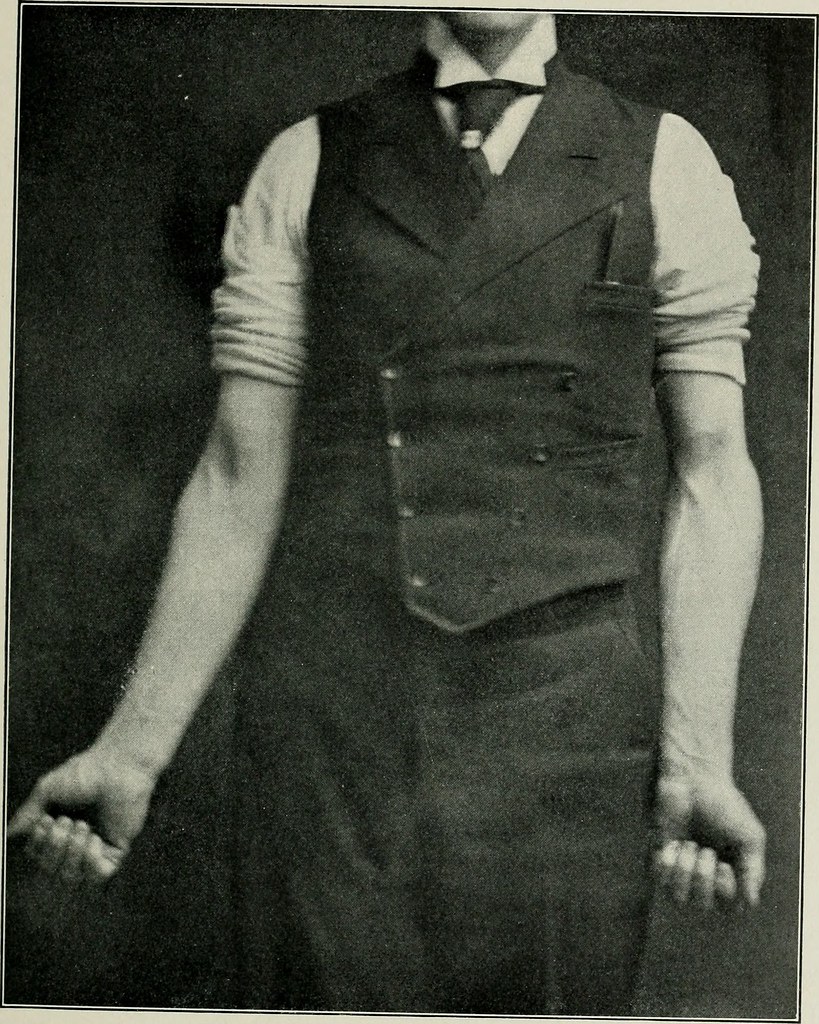
Ask the patient to stand with their forearms supinated by their side in the anatomical position. Demonstrate the pose for the patient to copy.
Position your patient in the anatomical position.
Anterior inspection
Observe the patient from the front for:
Muscle bulk and symmetry: Inspect the bulk of the deltoid, quadriceps femoris and in males, the pectoralis muscles. Changes in the muscle bulk may indicate wasting following injury or nerve damage but can also be natural (a tennis player for example, may have asymmetric muscle bulk in their upper limbs).
Joint alignment: Injuries can lead to joint misalignment. For example, a supracondylar fracture of the humerus can result in cubitus varus, also known as a “gunstock deformity.”
Iliac crest level alignment: The iliac crests should lie at an equal horizontal level. Misalignment can occur in pregnancy or injury which results in iliac subluxation.
Toes: Observe for any evidence of toe clawing (toes are held in flexion at the metatarsophalangeal [MTP] and interphalangeal joints), hallux varus (medial deviation of the great toe at the MTP joint) or hallux valgus (lateral deviation of the great toe at the MTP joint).
A varus deformity describes an inward angulation in which the lateral segment of a joint is deviated medially. In a valgus deformity, there is an outward angulation in which the lateral segment of a joint is deviated laterally
The sacroiliac joint acts as a shock absorber during walking and it is stabilised by many ligaments. In pregnancy these ligaments can become lax.
Spinal alignment: A small amount of cervical lordosis, thoracic kyphosis, and lumbar lordosis is expected. Excessive thoracic kyphosis (hyperkyphosis) is may be due to posture, age, or pathologies such as osteoporosis.
Knee and elbow joint extensibility: Inspect the knee and elbow joints for hyperextension or a fixed flexion deformity. Hyperextension at the knees and elbows can occur with collateral ligament damage or may point towards hypermobility syndrome. Those with a fixed flexion deformity will be unable to fully extend their joint to 180°. This may be congenital or acquired following trauma or inflammatory disease.
Foot arch: Take a closer look at the patient’s feet and observe for any pes planus (flat foot arch) or pes cavus (pronounced foot arch).
Patients can have lax (stretchy or long) ligaments which allow for excessive joint mobility eventually leading to a hyperextended appearance. The resulting instability can increase the risk of joint dislocation.
Muscle bulk and symmetry: Inspect the shoulders, gluteus, and calves. Changes in the muscle bulk may indicate the presence of pathology but can also be natural as mentioned above.
Spinal alignment: Observe for any scoliosis (lateral curvature of the spine).
Knee swelling: Look behind the knees in the popliteal fossa for any visible swellings that may be present such as a popliteal cyst or aneurysm.
Varus/valgus deformity of the knee/lower limb: Varus deformity of the knee describes a bowing appearance whereas in a valgus deformity the patient’s knees will “knock” together.
Varus/valgus deformity of the ankle: A varus/valgus deformity can also be observed at the ankle joint. This is best observed by looking at the achilles tendon, where you may see a medial displacement (valgus deformity) or lateral displacement (varus deformity) of the hindfoot.
Ask the patient to walk for 5m, turn around, and then walk back. Assess the gait for:
Smoothness: A jittery gait may suggest the presence of a tremor and/or cerebellar disease.
Symmetry: Asymmetrical gaits tend to occur with unilateral pathology, that is, when one lower limb is affected greater than the other. For example, in an antalgic gait on order to minimise weight-bearing on the affected limb, there will be a lengthened swing phase (see the complex-box below) on that side, with a shortened phase in the contralateral limb.
Speed: A slowed gait can occur in individuals suffering from musculoskeletal disorders of the lower limb. Antalgic gaits are often slow, as are gaits in those with Parkinson’s disease.
Stride length: A decreased stride length may be neurological, such as with the shuffling gait in Parkinson’s disease.
Ability to turn: If a patient has a slowed or unstable turn this is important to pick up on as this affects their ability to maintain independence.
First five phases of the gait cycle - left lower limb.
1. Heel strike: The initial contact of the heel with the ground. 2. Foot flat: Weight is transferred onto the foot. 3. Mid stance: Body alignment and balancing of weight on the foot. 4. Heel off: Heel lifts off the ground with the toes still touching the ground. 5. Toe off: The toes lift off the ground and the foot is no longer in contact. 6. Swing: The leg swings forward in preparation of the heel strike of the next step.
Upper motor neurone associated gaits:
If there's a unilateral lesion, there will be circumduction of the leg on the affected side, with the leg dragging behind the patient in a semi-circular fashion. This is known as a circumduction or hemiplegic gait. It occurs because hypertonia in an UMN legion causes flexion of the pelvis, hip and legs, which produces a crouching-like posture. The adductors are tight, pushing the knees together. If both legs are affected (bilateral lesion), the knees approach each other evern closer and can often cross with each step, producing a "scissoring gait".
Lower motor neurone associated gaits:
In a peripheral motor neuropathy, there will be muscle wasting and loss of function in the affected leg(s), and this may have an impact on gait. For example, injuries to the L5 nerve root or the common peroneal nerve will result in a relative inability to dorsiflex at the ankle joint (foot drop). Whilst walking, the patient will naturally attempt to compensate for this by raising their leg higher, resulting in a high stepping gait.
Peripheral sensory neuropathy associated gaits:
Sensory neuropathies may affect all modalities, including light touch, pain, temperature, vibration sense and proprioception. As a result, patients often lose their balance easily. To steady themselves, they spread their legs apart, resulting in a broad-based gait. Additionally, patients will not know what force to use when in contact with the ground, and will often exaggerate their step, resulting in a stamping gait. They rely on their sight to aid with walking, and therefore Romberg's test will be positive.
Myopathy and myasthenia gravis associated gaits:
Myopathies affect muscles more proximally (closer to the spine), particularly the hip abductors. If this occurs bilaterally, then there will be then there will be a "hip drop" on both sides leading to a waddling gait.
If however only one set of hip abductors is affected, for example due to trauma to the muscles or the corresponding superior gluteal nerve, then, when the patient raises their contralateral leg (the side without the lesion), their hip will unilaterally drop on the uninjured side (sound side sags). This phenomenon, known as Trendelenberg's sign, will produce a special gait known as Trendelenburg's gait.
Cerebellar gait:
Patients with cerebellar lesion have a lack of coordination, resulting in a characteristic cerebellar or ataxic gait. Features of such a gait include a broad-base, irregular steps and swaying. See the cerebellar examination page for more details.
Parkinsonian gait:
Patients will have a stooped posture with a reduced arm swing and a narrow-based, shuffling gait. They will take short, accelerating steps, which is referred to as a festinating gait.
Early on, patients may present with just the reduced arm swing on one side. This may be elicited this by lightly rocking the patient's shoulder side to side to see if both arms swing equally.
Antalgic gait: The patient walks in a manner to avoid pain. They will have a lengthened "swing phase" and will attempt to reduce weight bearing on the affected leg.
Upper limb (arms)
Arm
Ask the patient to stand in front of you and carry out the following two movements to assess their arms. Patients suffering with rotator cuff injuries may struggle or experience pain with these tasks:
1. Ask the patient to place their hands behind their head and flare out their elbows. This crudely assesses external rotation and abduction of the shoulder as well as flexion of the elbow.
2. Ask the patient to place their hands behind the small of their back. This crudely assesses >internal rotation and adduction of the shoulder as well as flexion of the elbow.
Demonstrating the movements and asking the patient to copy you is generally a smooth and slick way of helping the patien to understand what to do. In addition, patients with hearing difficulties will have a much easier experience.
Hand
Inspection
Ask the patient to extend their arms out and face their palms downwards.
Look at the back of the hands for:
Muscle wasting:Wasting in the dorsal interosseous space suggests an ulnar nerve or spinal root injury.
Joint swellings:Bouchard's and Heberden's nodes are both found in osteoarthritis.
Joint deformities:Ulnar deviation, bountonnière and swan neck deformities can all be found in rheumatoid arthritis.
Visible masses: Check the dorsum of the wrist for a ganglion cyst.
Ask the patient to turn over their hands and observe the palmar aspect for:
Muscle wasting:Wasting in the thenar eminence occurs in carpal tunnel syndrome.
Palmar fascial swellings: Inspect the fingers for Dupuytren's contracture and trigger finger deformities.
sing your index finger and thumb, squeeze the metacarpophalangeal (MCP) joints of each of the patient’s hands whilst observing their face to assess for pain. This will usually occur in patients with inflammatory arthritis or traumatic injury to the hand.
Power
Assess the power of the muscles in each hand. Multiple movements can be tested here, however only the following four are necessary:
Digit abduction: Ask the patient to abduct their fingers against resistance. Be sure to use the same fingers as the patients to resist. This will test the dorsal interossei muscles. Damage to the intrinsic muscles of the hands can result in decreased ability to abduct or adduct the fingers.
Digit adduction: Ask the patient to hold a piece of paper between any two fingers. Using the same fingers, attempt to pull the paper from the patient and ask them to resist. This will test the palmar interossei muscles.
Power/palmar grip: Ask the patient to squeeze your finger to assess their power grip. This is an important functional grip and that uses the muscles of the anterior and posterior forearm compartments. Grip strength can be reduced for many reasons in patients including joint deformities, contractures and nerve injury.
Precision/pincer grip: Ask the patient to tap each of their fingers on their thumb to assess the coordination of their pincer grip. Next, attempt to break their grip with a pincer grip of your own and ask the patient to resist.
Lower limb (legs)
Instruct the patient to lie on the bed set flat at 180°
Knee
With one hand on the patient’s knee and the other at the base of the patient’s foot, passively flex each knee and assess for range of movement and crepitus. Knee crepitus is a common finding in patients with osteoarthritis of the knee.
Patellar tap test
Perform the patellar tap test on each leg to test for an effusion. Keep the knees extended and glide your hand down the patient’s thigh to squash the suprapatellar pouch. This pushes an effusion, if present, out of the pouch and behind the patella. Utilising two fingers of the other hand press downwards gently on the patella itself. The test will be positive if the patella bounces and taps.
Feet
Inspection
In a similar manner to the hands, inspect the patient’s feet for any swellings, deformities or callosities that may be present.
Palpation
Squeeze the MTP joints of each of the patient’s feet whilst observing their face to assess for pain. Patients with inflammatory arthritis, gout, or traumatic injury to the foot may experience pain on MTP palpation.
Spine
Ask them to stand upright one more, but this time place your index fingers on the lumbar spine roughly 10 cm apart. Instruct the patient to lean forwards as if to touch their toes. As they flex their back, crudely assess for lumbar extension. Expect extension of approximately 5cm. An extension of <5cm is indicative of a decreased range of movement and should be confirmed accurately using Schöber’s test.
Stand facing the patient and ask the patient to follow your movements. Patient’s suffering from conditions such as ankylosing spondylitis, osteoarthritis, discitis or other spinal pathologies will have limited range of movement when asked to carry out these tasks.
Ask the patient to slide their hand down your side to laterally flex their spine. Repeat this on the other side.
Ask the patient to place their ear to their shoulder to assess lateral flexion at the neck. Repeat on the other side.
Ask the patient to place their chin to their chest to assess neck flexion.
Ask the patient to place their chin towards the ceiling to assess neck extension.
Completion
Present your findings or record them in the patient notes.
QGOSAL Some students utilise this alternative method as a tool to guide them through the GALS OSCE to ensure they cover each main heading from the examination.
Questions Gait Observations Spine Arms Legs.
This method minimised patient movement, allowing for a smoother examination.
Additional examinations
If there were any notable findings from your GALS screen, or the patient complained of any symptoms, proceed to perform the relevant regional examination of the musculoskeletal system (REMS). Ideally after this point, to complete your examination you should closely examine the joint above and the joint below the REMS joint. In an examination, you will probably be stopped by the examiner at this point.
Following the complete examination (including REMS if necessary), thank the patient for allowing you to examine them and offer to help them get dressed and ensure they are comfortable.
Interactive markscheme
When assessing each other, click on each list item as you go along. Doing so will turn the list item green. Make careful note of any steps missed at the end. We recommend completing any examination or procedure in under 10 minutes, but you can adjust the timer to suit your needs.
:
Introduction: “Hello, I’m SimpleOSCE and I am a medical student. I've been asked to do a screening examination of your body to check the function of your muscles and joints, would that be ok? Can I confirm your name and DOB? Thank you.”
Obtain consent and ensure adequate exposure.
Wash your hands.
Ask if the patient is in any pain.
Perform a general inspection of the patient and around the bed.
Screening questions
Ask the patient: "Do you have any pain or stiffness in any of your joints, in your muscles, or in your back?".
Ask the patient: "Do you experience any difficulty with walking up and down stairs?".
Ask the patient: "Do you experience any difficulty with dressing yourself in the morning?"".
Closer inspection
Observe the patient from the front for muscle bulk and symmetry, joint alignment and foot deformity.
Observe the patient from the side for spinal alignment, knee and elbow joint extensibility and foot deformity.
Observe the patient from the back for muscle bulk and symmetry, joint alignment and knee/ankle swelling and deformity.
Gait
Assess the patient's gait.
Upper limbs ("Arms")
Ask the patient to place their arms behind their head and flare out their elbows.
Ask the patient to place their hands behind the small of their back.
Inspect the dorsal and palmar surfaces of the hands.
Palpate the metacarpophalangeal joints.
Assess finger abduction and grip strength.
Lower limbs ("Legs")
Flatten the bed to 180°.
Assess the knee joint for range of movement and crepitus.
Perform the patellar tap test.
Inspect the feet for callosities and deformities.
Palpate the metatarsophalangeal joints.
Spine
Ask the patient to stand and lean backwards.
Assess for lumber extension.
Completion
Thank the patient and present your findings to the examiner.
If indicated, state that you wish to perform a regional examination of a specific joint in addition to the joint above and below.


.jpg)




_(14578123550).jpg)

_(14781017221).jpg)
]")



